
Anterior cruciate ligament (ACL) injuries are a common setback for athletes, particularly in dynamic sports like soccer. Alarmingly, 88% of ACL injuries occur without direct contact, typically during high-demand movements like single-leg deceleration, cutting, jumping, or pivoting. After ACL reconstruction (ACLR), the return-to-sport (RTS) phase is a critical milestone, but traditional testing protocols may overlook key deficits that persist post-rehabilitation.
A recent study by Kotsifaki et al. (2023; 2021) sheds light on the limitations of conventional hop tests and presents a compelling case for integrating vertical jump testing into RTS assessments.
Limitations of Traditional Hop Testing
Criteria-based rehabilitation is the gold standard for guiding RTS decisions. Athletes are often cleared based on strength testing and a battery of hop tests that assess functional symmetry between the injured and uninjured limbs. While these tests are widely accepted and easy to implement, their ability to predict successful RTS and prevent re-injury remains questionable.

Key limitations of hop tests include:
- Overestimation of Rehabilitation Progress: Achieving symmetry in hop distance, measured via the Limb Symmetry Index (LSI), often occurs earlier in the recovery process than symmetry in isokinetic knee strength. This can give a false sense of readiness.
- Limited Insight into Knee Function: Hop distance alone doesn’t capture the biomechanical deficits or compensatory strategies athletes develop to protect the reconstructed knee.
- Persistent Risk of Re-Injury: Studies show that despite meeting RTS criteria, re-injury rates range from 20-30% within two years, likely due to unaddressed deficits in neuromuscular control and strength.
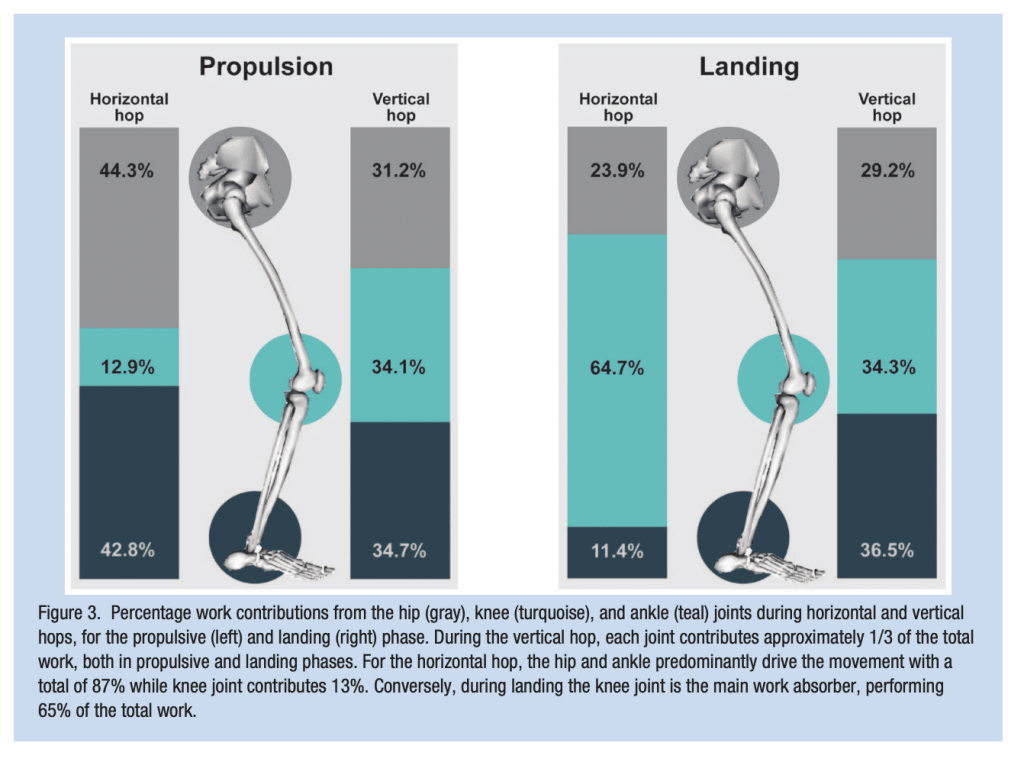
Due to the nature of horizontal hop testing, they largely capture and assess the propulsion phase of hopping. We know that in the propulsion phase of horizontal hopping the hip, knee, and ankle contribute 44%, 12%, and 42%, respectively of the work. These limitations highlight the need for more robust evaluation tools that assess knee function comprehensively.


Why Vertical Jump Tests May Be Superior
Vertical jump testing offers deeper insights into lower-limb power, reactivity, and biomechanical symmetry, especially when it comes to the knee joint—factors often overlooked by horizontal hop tests. Comparatively, the vertical jump hip, knee, and ankle contribute 31%, 34%, and 34% of the work, respectively.
The study by Kotsifaki et al. examined 48 male participants, including 26 post-ACLR athletes that were cleared for RTS and 22 healthy controls. Testing protocols included single-leg vertical jumps and single-leg drop jumps, focusing on joint motion, muscle activation, and work distribution across the hip, knee, and ankle.
Key findings include:
- Performance Deficits: Post-ACLR athletes exhibited significantly lower jump height and reactive strength index (RSI) in the involved limb compared to the uninvolved limb and control group.
- Work Distribution: Athletes offloaded the injured knee during propulsion and landing, increasing hip work. This compensatory strategy highlights persistent deficits in knee function.
- Biomechanical Alterations: Altered landing mechanics, such as extended knee positions, increased hip flexion, and trunk deviations, were observed. These changes may elevate re-injury risk.
- Muscle Activation Patterns: Post-ACLR athletes showed increased hamstring activation and reduced soleus contribution, indicating altered neuromuscular strategies.

The Case for Jump Height and RSI
Metrics like jump height and RSI focus on the concentric phase of movement, which requires powerful, coordinated hip, knee, and ankle extension. Healthy individuals rely on the knee for approximately three times more work during vertical jumps than horizontal hops, emphasizing the knee’s critical role.
Post-ACLR athletes, however, demonstrated:
- Jump Height Symmetry: Only 77-83% compared to their uninvolved limb.
- Work Symmetry: 70-75% during vertical jumps, well below the near-perfect symmetry of controls.
These deficits persisted even in athletes who passed traditional hop test criteria, reinforcing the need for vertical jump tests in RTS assessments.

Implications for Rehabilitation
This study underscores the importance of rethinking RTS assessments and rehabilitation approaches:
- Incorporate Vertical Jump Testing: These tests are more sensitive to knee-specific deficits and provide valuable data on power and biomechanical asymmetries. Additionally, the vertical jump tests may be easily implemented and measured
- Address Deficits Beyond Hop Distance: Focus on enhancing lower-limb power, reactive strength, and neuromuscular control, particularly in the soleus, which plays a pivotal role in reducing ACL loading.
- Correct Compensatory Strategies: Rehabilitation programs must prioritize balanced work distribution across the hip, knee, and ankle to minimize re-injury risks.
- Consider Gender Differences: Female athletes often demonstrate different compensation strategies, such as greater reliance on quadriceps or hip mechanics, which should guide individualized interventions.
Final Thoughts
Although traditional methods of horizontal hop testing for time or distance may fail to capture the function of the key joint, they do have face validity. Interestingly and undoubtedly, horizontal hop testing does have a very important component. The landing. The landing and stopping phase of horizontal hop testing has two important factors that make it very interesting from a rehab and clinical perspective. 1) massive face validity with stopping or change of direction from athletic movements and 2) in the landing phase of horizontal hop testing the distribution of work favors the knee and muscles surrounding it. The work contribution of the landing phase of the horizontal hop test for the hip, knee, and ankle is 23%, 64%, 11%, respectively; making the assessment of the horizontal landing phase potentially interesting from a clinical discharge criteria perspective.
Vertical jumps can be quickly and easily accessed via measurement of height making it an easily administered test with a higher chance of capturing important asymmetries before athletes return to sport. But the combination of these tests may raise important questions to understand compensation strategies post ACLR. For instance, if an athlete clears the hop testing, but not vertical jump tests, is the athlete adopting a hip strategy? On the other hand what if an athlete fails to clear the horizontal hop test and passes the vertical jump test does that mean tha athlete adopts a more knee dominant strategy in their propulsion? What is the best way to measure how athletes land?
ACL injuries occur in mere milliseconds but demand months—or even years—of recovery. By incorporating vertical jump testing into RTS protocols, clinicians can gain a more comprehensive understanding of knee function and neuromuscular readiness. While no testing protocol can guarantee injury prevention, addressing these persistent deficits is a step toward optimizing recovery, reducing re-injury risk, and ensuring athletes are truly ready to return to play.
Radek Wiechecki
Physiotherapist
References:
- Kotsifaki, R., Sideris, V., King, E., Bahr, R., & Whiteley, R. (2023). Performance and symmetry measures during vertical jump testing at return to sport after ACL reconstruction. British Journal of Sports Medicine, 57(20), 1304-1310
- Kotsifaki, A., Korakakis, V., Graham-Smith, P., Sideris, V., & Whiteley, R. (2021). Vertical and horizontal hop performance: contributions of the hip, knee, and ankle. Sports health, 13(2), 128-135.